OFFICE HOURS |
OFFICE INFORMATION |
||
|
Monday - Friday |
8:30am - 4:30pm |
980 Westfall Road |
[Phone] 585.442.1110 |
 |
I Would Like To:
|


Correction of Vocal Cord Paralysis
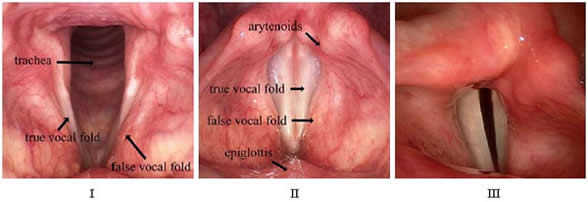
The voice box, or larynx, has three important functions. It is necessary for breathing, voice and
swallowing. The vocal folds have two positions, open (apart) for breathing (picture I) and closed (together) for
making sound, coughing and sealing off the lungs when swallowing (picture II). When one of the vocal folds are
paralyzed, it usually rests in an in-between position (picture III), and neither opens for breathing, nor closes
for voicing, coughing, or swallowing. Usually, the effects on the voice are
the most dramatic. The voice becomes weak
and breathy. People can only say a few words per breath, and are frequently
out-of-breath, or physically tired when
trying to speak for more than a few minutes straight. The voice may also get somewhat high and squeaky, with a
diminished range. Swallowing may be affected as well, where you may notice some choking or coughing with certain liquids. Your cough is frequently different and very weak. This is a serious problem for patients with with vocal fold paralysis because one of the most important functions of the larynx is to keep liquids out of the lungs, and to be able to cough up mucus. When this does not happen, you are at risk for getting an "aspiration" pneumonia. The surgical procedure to restore these important functions is called "medialization laryngoplasty"
Medialization Laryngoplasty
What does medialization laryngoplasty aim to accomplish?
Voice: power & projection would be significantly improved. You should be able to say many more words per breath, and be less fatigued when speaking the high squeakiness should be decreased, and your range would be better. You should notice a difference almost as soon as you wake up from the procedure. The final results take about six weeks, when all of the swelling from the surgery resolves. Expect a "surgical laryngitis" (hoarseness) for the first few weeks.
Swallowing & Cough: less choking on liquids, and a stronger, more effective cough
overall, a safer, more 'competent' larynx
What is medialization laryngoplasty?
"Medialization" (moves to the middle) "laryngoplasty" (reconstruction of the voice box) aims to restore function to the larynx by moving the paralyzed vocal fold to the middle. When this occurs, the un-paralyzed side meets it in the middle for non-breathing functions, and results in complete closure. As above, complete closure is necessary for making sound, coughing and sealing off the lungs when swallowing. Therefore, these functions are mostly restored! A common concern is if the breathing is significantly altered by moving the vocal fold to the middle? The answer is: not really. A professional athlete who uses every millimeter of their airway when breathing will be aware of a 5-10% reduction in airway capabilities. The rest of us generally do not, and when so, it is a very subtle difference noticed only when vigorously exercising. If we consider the gains in voice, cough and swallowing function, versus the 5-10% loss in airway capabilities, your overall health and well-being would significantly benefit from medialization.
There are two types of medialization laryngoplasty: injection, and implant. The injection may be done in the clinic with local anesthesia or in the operating room under general anesthesia. The advantages of a clinic-based procedure is avoidance of general anesthesia and a trip to the operating room, however, clinic-based injection procedures may be less effective at voice restoration versus a vocal cord implant, and generally do not positively impact swallowing.
The permanent implant is done in the main operating room, as "day surgery" (you go home the same day). It is done with intravenous anesthesia, where you will feel and remember nothing, but a breathing tube is NOT placed. A small incision is placed in a skin crease over the larynx. A 'window' is drilled out of the larynx, providing access to the paralyzed vocal fold. I will then place a hand-carved implant made out of a surgical polymer. Once inserted, I verify the size and placement of the implant by looking with a scope, and make any necessary adjustments. During the 'looking part' of the operation, we will lighten the anesthesia, and ask you to make sounds. Once verified, the anesthesia will be deepened, and everything is sutured.
Arytenoid Adduction
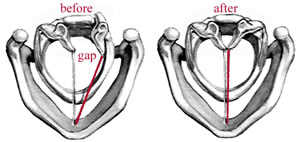
Sometimes the gap between the vocal folds is too great to be closed with an implant alone. Additionally, a very large gap can significantly impair the swallowing, with liquids frequently going down the "wrong pipe." In these cases, it may be preferable to move the cartilage of the vocal cord as well as placing an implant. This procedure is called an arytenoid adduction, and is done in conjunction with medialization laryngoplasty. In contrast to just placing an implant (medialization laryngoplasty), repositioning the cartilage (arytenoid adduction) is much more involved because this cartilage is on the back side of the voicebox. The goal of the procedure is to move the vocal cord cartilage into the middle, closing the gap between the vocal cords which contribute to to the voice and swallowing problems (see diagram below).
To reach this cartilage, a longer incision must be used, and many of the large muscles of the neck must be divided and then later sewn back together. As such, the severity and duration of post-operative discomfort is significantly greater, lasting upwards of a week. The length of the procedure also increases from 60-90 minutes for an implant alone to 2-3 hours for an implant + cartilage repositioning, and a 1-2 day post-operative hospitalization is required. Unfortunately, an arytenoid adduction is sometimes the only way in which to close the vocal cord gap sufficiently to achieve a reasonable voice, restore a strong cough, and reduce swallowing difficulties. The pros and cons of adding an arytenoid adduction to medialization laryngoplasty is individual, and is discussed in detail during consultation.
Post-Operative Instructions
Medialization laryngoplasty (implant) alone:
You will have steri-strip bandages over the2-inch incision post-operatively, which should be left alone and kept dry. You may bathe, and wash your hair, but may not shower or get the incision wet until your one-week post-operative visit. Getting the incision wet increases the chances of infection. If the implant gets infected, you may end up with scarring, potential need for more surgery and possibility of an irreversibly worse voice than what you had preoperatively. You will be given an antibiotic to take for five days post-operatively to start on the day AFTER surgery. If the incision get red or starts draining, or is associated with pain that is increasing you should call the office immediately.
You may be given different (sometimes conflicting) post-operative instructions regarding your voice. There is NO voice restriction or voice rest. You should notice a difference almost as soon as you wake up from the procedure, however, the final results take about six weeks for all of the swelling from the surgery to resolve. Expect a "surgical laryngitis" (hoarseness) for the first few weeks-months.
There are no dietary restrictions. You are on a "see-food" diet. If you "see food" and want to eat it, then eat it!
Extra-strength tylenol or ibprofen may be used for any post-operative discomfort. If something stronger is needed, it is usually a sign of something unusual. We are happy to provide something stronger, however, you will need to telephone the office so that you can be evaluated.
No lifting anything heavier than a gallon of milk for one week. You may lightly exercise as long as you are neither lifting weights, nor exercising to the point of sweating (as you must keep the incision clean and dry). Typically one week off from work / school is given post-operatively to recover.
Medialization laryngoplasty (implant) WITH arytenoid adduction (cartilage repositioning):
There will be a surgical drain in the wound following the surgery which will be painlessly removed the next morning in the hospital. As above, it is critical that the incision remains clean and dry. You will go home with a temporary
bandage which may be removed on the following deay upon returning home from the hospital. The incision may leak a little for the first 24 hours after the drain is removed ... this is normal.
As above, there is no voice rest or swallowing restrictions, however, most have some discomfort when swallowing after the cartilage repositioning because of the muscles that had to be divided and sewn back together. If a softer or liquid diet feels better for the first few days, this is expected and allowed. Your body and common sense will dictate when it is advisable to begin a normal solid-food diet.
Strong pain medication, steroids (to reduce swelling on the inside) and antibiotics will be given post-operatively. All three are important to speed the healing. The codeine based pain medication may be alternated every two hours with ibprofen, if necessary. Call with any questions or concerns regarding how to take your medication.
Video
Watch a video of vocal cord paralysis before repair. Note the persisting gap between the vocal cords as they try to close.
Watch a video of the same vocal cord paralysis after repair. Note the gap is eliminated.